What does bilateral JVD indicate
By Andrew Hansen
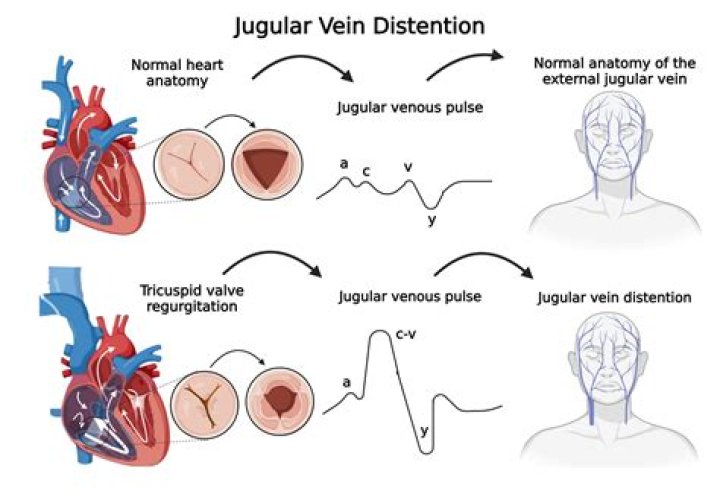
JVD is a sign of increased central venous pressure (CVP). That’s a measurement of the pressure inside the vena cava. CVP indicates how much blood is flowing back into your heart and how well your heart can move that blood into your lungs and the rest of your body.
What causes bilateral jugular vein distention?
Yes, heart disease is the most common cause of JVD, including arrhythmia (irregular heart rhythm), atherosclerosis (a buildup of fat, cholesterol, and other substances in the artery walls), cardiomyopathy (heart muscle disease), congenital heart defects, coronary artery disease, and infections.
What does jugular venous pressure indicate?
Elevated jugular venous pressure is a manifestation of abnormal right heart dynamics, mostly commonly reflecting elevated pulmonary capillary wedge pressure from left heart failure. 12. This usually implies fluid overload, indicating the need for diuresis.
What do distended neck veins indicate?
In patients with acute inferior-wall MI with right ventricular involvement, distention of neck veins is commonly described as a sign of failure of the right ventricle. Impaired right ventricular function also leads to systemic venous hypertension, edema, and hepatomegaly.Why do we assess for JVD?
Its most common use is to estimate the right atrial pressure, especially in patients with heart failure, and also to measure the response to diuretic therapy. It is also helpful in the evaluation of conditions such as superior vena cava obstruction, tricuspid valve disease, and pericardial disease.
Does a pneumothorax cause JVD?
Thus, a tension pneumothorax creates not only a respiratory compromise but also a cardiovascular compromise. Tension pneumothorax presents with respiratory distress, jugular venous distention (JVD), diminished breath sounds, tachycardia and narrow pulse pressure.
What causes JVD in heart failure?
Common causes of jugular vein distention Congestive heart failure (deterioration of the heart’s ability to pump blood) Constrictive pericarditis (infection or inflammation of the lining that surrounds the heart that decreases the lining’s flexibility) Hypervolemia (increased blood volume)
How do you evaluate JVD?
To properly evaluate jugular venous distension, the patient must be placed at a 45-degree angle, or slightly less. Visualization of the jugular veins is best done at an oblique angle, so sit beside the patient and elevate the head of the cot into a semi-Fowler’s position.What conditions cause JVD?
JVD is often caused by life-threatening conditions such as pulmonary embolism, tension pneumothorax, car- diac tamponade, and heart failure,1 and is a classic and crucial finding in the evaluation of all patients presenting with shock.
How do nurses test for JVD?Measure the height of the bulge or distention of the jugular vein. Ask the patient to lie down on the exam table with the head at 45 degrees. Ask him/her to turn his/her head to the side to measure the central venous pressure (CVP). The physician will measure the height of the bulge of JVD to indicate CVP.
Article first time published onIs visible JVP normal?
Normally only the a and v waves are visible. Conditions associated with an elevated JVP include congestive heart failure and fluid overload.
Why does jugular venous pressure decrease during inspiration?
JVP normally decreases during inspiration because the inspiratory fall in intrathoracic pressure creates a “sucking effect” on venous return. Thus, the Kussmaul sign is a true physiologic paradox. This can be explained by the inability of the right side of the heart to handle an increased venous return.
Is an EJ a central line?
Central venous cannulation via the external jugular vein (EJV) is a recognized technique [1-3]. It is associated with minimal complications but with a relatively frequent failure rate compared with the cannulation of the internal jugular or subclavian veins (SCV) [1,3,4].
How serious is JVD?
JVD can be the sign of a severe condition, including heart failure, so it is vital that a person is seen by a medical professional as soon as possible. While heart failure can happen to anyone, risk factors for heart failure include: high blood pressure.
Which symptom is most commonly associated with the left-sided heart failure?
The symptoms of left-sided heart failure are the generally the same for heart failure broadly and include: Shortness of breath. Difficulty breathing when lying down. Weight gain with swelling in the feet, legs, ankles.
Which of the following symptoms is most commonly associated with left-sided heart failure?
Left-sided heart failure symptoms include: Awakening at night with shortness of breath. Shortness of breath during exercise or when lying flat. Chronic coughing or wheezing.
How is Hemothorax diagnosed?
Share on Pinterest A hemothorax may be diagnosed with an X-ray or a CT scan. During a physical exam, doctors will listen for sounds of abnormal breathing through a stethoscope. Doctors may also tap on the chest to listen for sounds of liquid.
How do you treat a Hemothorax in the field?
Treatment of a hemothorax includes supportive care, high-flow oxygen, two large-bore intravenous (IV) lines, and transport. Keep in mind, a needle decompression of a hemothorax is an absolute contraindication.
Is atelectasis serious?
Large areas of atelectasis may be life threatening, often in a baby or small child, or in someone who has another lung disease or illness. The collapsed lung usually reinflates slowly if the airway blockage has been removed. Scarring or damage may remain. The outlook depends on the underlying disease.
When does S3 occur?
The third heart sound (S3), also known as the “ventricular gallop,” occurs just after S2 when the mitral valve opens, allowing passive filling of the left ventricle. The S3 sound is actually produced by the large amount of blood striking a very compliant left ventricle.
What is considered elevated JVP?
JVP is > 9 cm above the right atrium (> 4 cm above the sternal angle)
Which technique is most appropriate for a nurse to implement during the assessment of the abdomen?
AUSCULTATION is usually performed following inspection, especially with abdominal assessment. The abdomen should be auscultated before percussion or palpation to prevent production of false bowel sounds. When auscultating, ensure the exam room is quiet and auscultate over bare skin, listening to one sound at a time.
What does positive JVD mean?
JVD is a sign of increased central venous pressure (CVP). That’s a measurement of the pressure inside the vena cava. CVP indicates how much blood is flowing back into your heart and how well your heart can move that blood into your lungs and the rest of your body.
What is Y descent?
The y descent represents the abrupt termination of the downstroke of the v wave during early diastole after the tricuspid valve opens and the right ventricle begins to fill passively. Normally the y descent is neither as brisk nor as deep as the x descent.
What causes Pulsus Paradoxus?
Pulsus paradoxus results from alterations in the mechanical forces imposed on the chambers of the heart and pulmonary vasculature and is often due to pericardial disease, particularly cardiac tamponade and to a lesser degree constrictive pericarditis.
What is Pulsus Paradoxus?
Pulsus paradoxus is defined as a fall of systolic blood pressure of >10 mmHg during the inspiratory phase.
Is an EJ a PICC line?
External jugular peripherally inserted central catheters (EJ PICCs) are defined as catheters placed through the external jugular vein and advanced into position where the distal tip dwells in the lower one-third of the superior vena cava to the junction of the superior vena cava and the right atrium.
Can nurses put in EJ?
Yes, some of our nurses put EJ peripheral IVs in if we cannot get other access. We use 18g for EJs.
What is an EJ in medical terms?
External jugular vein cannulation is an integral part of modern medicine and is practiced in virtually every health care setting. … This topic describes placement of an intravenous (IV) catheter into the external jugular vein. A similar technique can be used for placement of IV catheters at different anatomic sites.